Growth or Stagnation? Oregon Faces Generational Choice
On its face, Oregon’s healthcare sector appears to be an economic bright spot. Data show hospitals, clinics, and social services are adding jobs even as other industries have struggled to recover from the pandemic. Oregon is also paying higher wages for healthcare workers on average compared to the rest of the country.
But according to Oregon Business Council President John Tapogna, the fact that healthcare is now carrying the state’s labor market should be a cause for concern, not celebration.
Speaking recently at the Oregon Health Forum, Tapogna argued that Oregon faces deeper challenges than the current business cycle. Population growth has largely stalled, housing costs remain stubbornly high, businesses face a comparatively heavy regulatory burden, and general skepticism toward growth has become embedded in policy.
Together, those long-term trends are making it increasingly difficult to attract new workers, grow businesses, and sustain a healthy economy, he said.
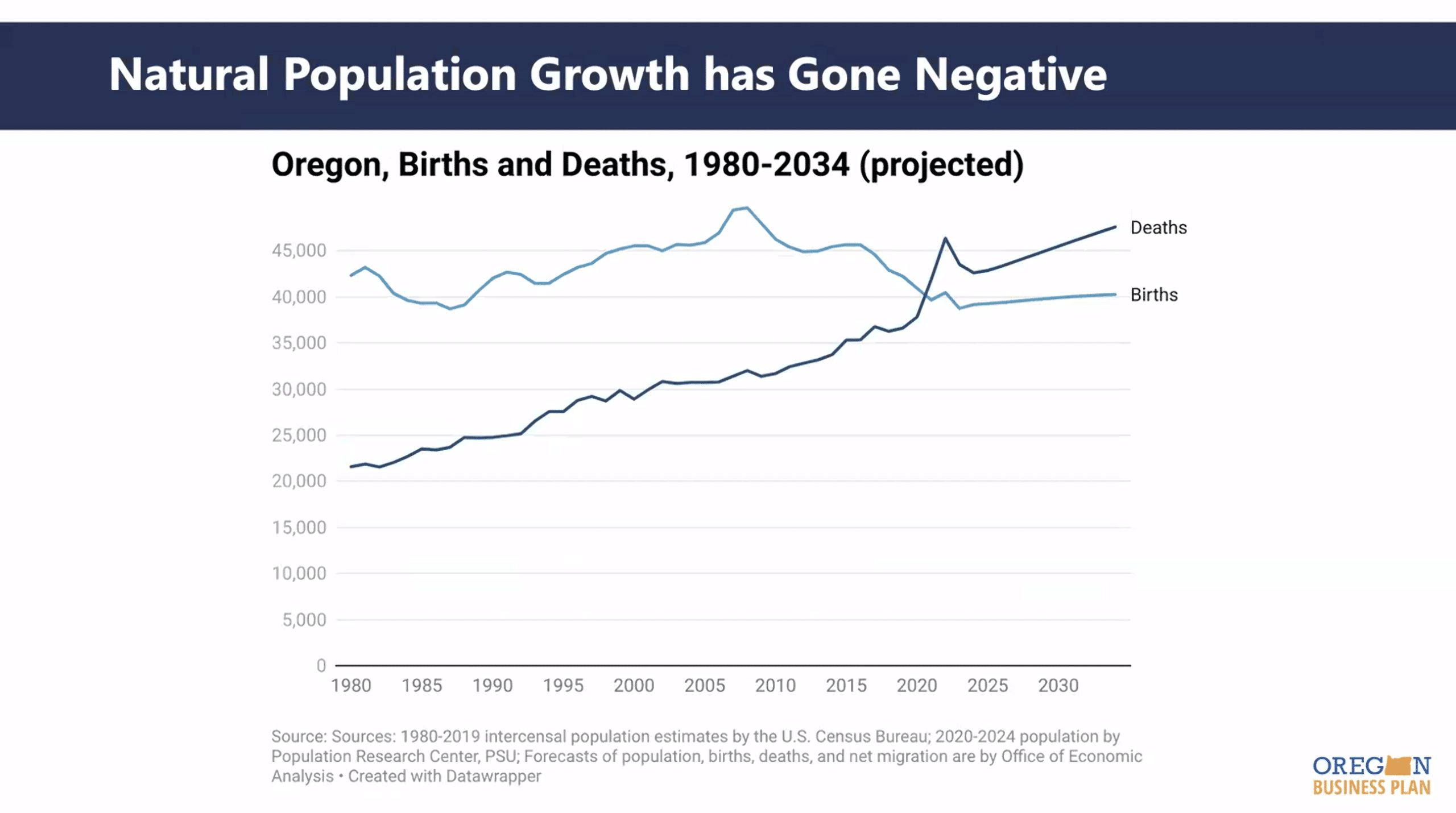
Population Stagnation
Oregon has now crossed into negative natural population, meaning more people are dying each year than are being born. Tapogna said the trend accelerated during the COVID-19 pandemic and leaves the state increasingly dependent on in-migration simply to maintain its current population.
Along with slowing population growth, Tapogna said Oregon’s gross domestic product has fallen off the national pace in recent years. While healthcare continues to add jobs, other traditional economic drivers are moving in the opposite direction. Manufacturing employment has slipped since the pandemic, and several metro areas including Portland, Albany, and Bend have experienced notable job losses.
“We have an aging population. We have healthcare needs … It’s OK and important for those (healthcare) sectors to be growing,” Tapogna said. “But in order to have a healthy economy, you want those other sectors to be growing along with it.”
Five Pressures
Tapogna identified five pressures pushing Oregon toward economic stagnation:
- High housing costs and homelessness, making it difficult for employers to recruit workers.
- Underperforming K-12 schools, despite increased spending.
- Increasing wildfire risk and smoke, discouraging growth in some parts of the state.
- Over-reliance on the individual income tax, especially in Portland.
- A deeply rooted cultural ambivalence toward growth that discourages investment.
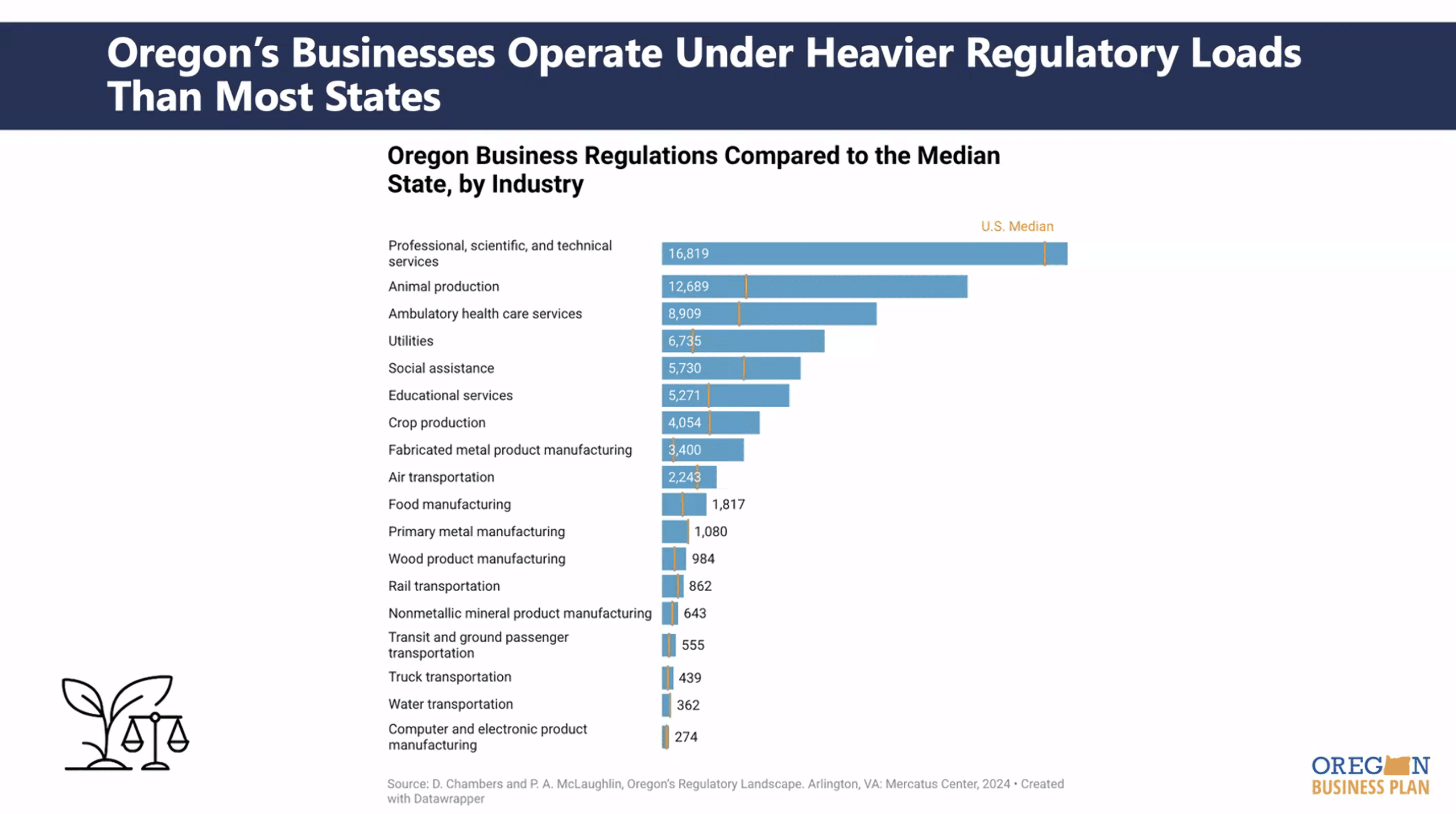
Housing costs are the main reason why businesses are struggling to attract talent, Tapogna said, though the tax and regulatory environment has also made it difficult for companies trying to expand.
Tapogna said the state is now leaning on the healthcare sector for job growth, which is quickly becoming strained. If the state goes through a period of very low growth or decline, he said it could make labor market challenges all the more painful.
Healthcare would feel those pressures first and most intensely, Tapogna said. A stagnant Oregon means tighter labor markets, greater fiscal strain, and more uninsured patients. The long-term sustainability of Oregon’s healthcare system, he said, will increasingly depend on whether the state can attract workers, families, employers, and investment.
“I think there’s a very strong case to be made that, at a minimum, the (healthcare) sector should be cheerleaders and participate in discussions around economic development going forward,” he said.
Prosperity Initiative
Looking at what the industry can do moving forward, Tapogna said there are two recommendations from the Governor’s Prosperity Council that stand out:
- Reduce regulatory and administrative burdens by 20% by 2029.
- Establish a Governor’s Cabinet of Economic & Talent Development.
The healthcare industry can participate by providing input on specific rules, workforce bottlenecks, regulatory delays, and measurable fixes, Tapogna said. He encouraged leaders to step up and help make the case for why Oregon should be prioritizing smart, intentional growth to avoid over-burdening the healthcare system.
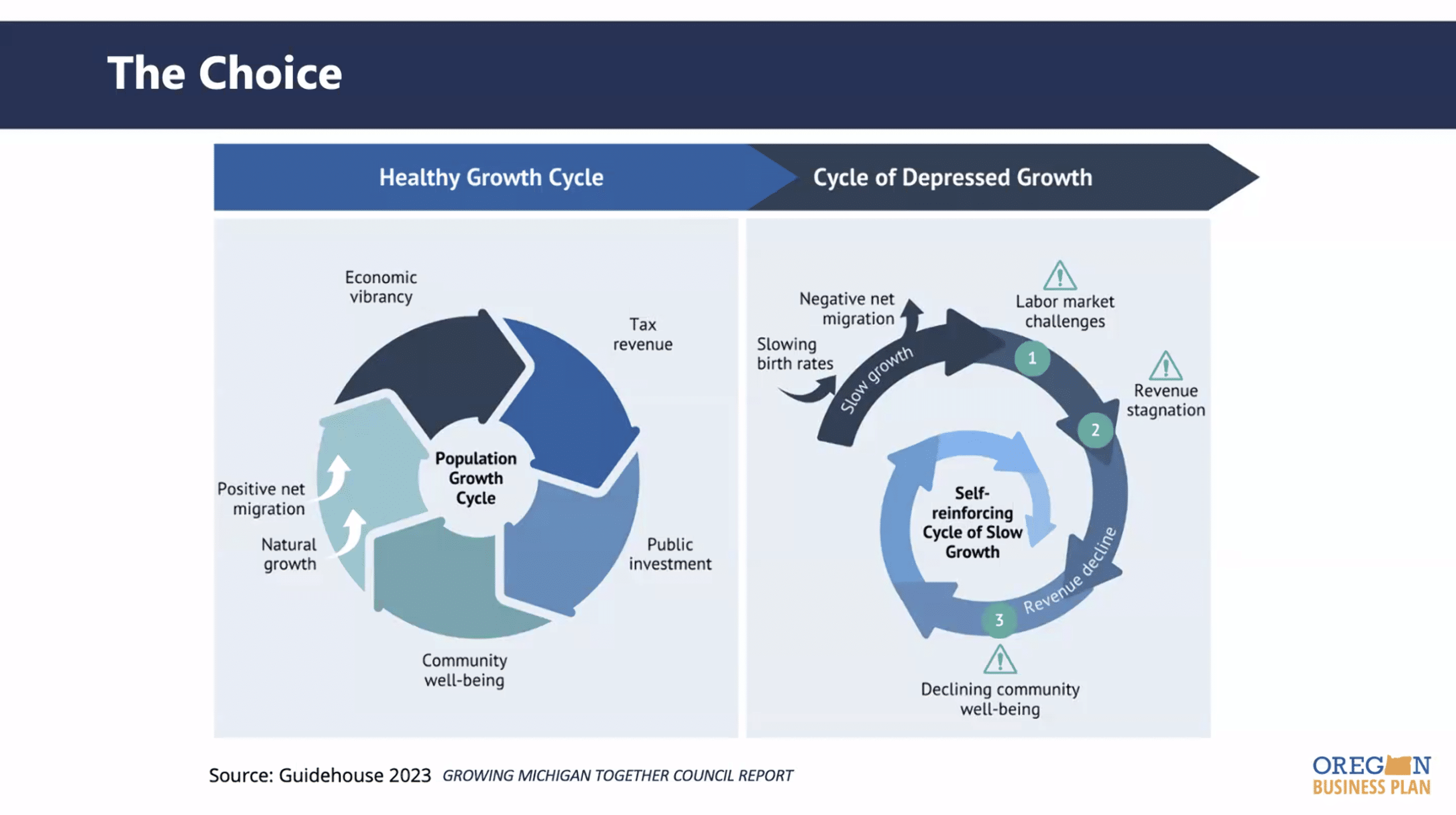
“Oregon has a choice between some intentional moderate growth, or flatlining and potentially declining in population over the next 10-20 years … Count me as a fan of moderate growth over stagnation or decline.”
— John Tapogna, President, Oregon Business Council